![]()
Original Article
Eduweb, 2026, enero-marzo, v.20, n.1. ISSN: 1856-7576
Doi: https://doi.org/10.46502/issn.1856-7576/2026.20.01.19
Integración de las tecnologías digitales en el desarrollo de la atención sanitaria entre los estudiantes de educación superior
Taisiia Komar
Doctor of Psychological Sciences, Professor, Head of the Department of Psychology and Pedagogics, Khmelnytskyi National University, Ukraine.
https://orcid.org/0000-0001-8957-0971
Oleksandr Martyniuk
Doctor of Philosophy in Public Management and Administration, Associate Professor of the Department of Border Security, National Academy of the State Border Guard Service of Ukraine named after Bohdan Khmelnytskyi, Ukraine.
https://orcid.org/0000-0002-0216-1356
Olha Oseredchuk
Doctor of Pedagogical Sciences, Professor at the Department of Practical Psychology and Mental Health, Institute of Law, Psychology and Innovative Education, Lviv Polytechnic National University, Ukraine.
https://orcid.org/0000-0002-3192-3129
Olha Tsviakh
PhD in Biology, Senior Lecturer of the Department of Physical Culture and Sport, Admiral Makarov National University of Shipbuilding, Ukraine.
https://orcid.org/0000-0002-1119-2170
Vitalii Borovskyi
Lecturer at the Department of Border Service, National Academy of the State Border Guard Service of Ukraine named after Bohdan Khmelnytskyi, Ukraine.
https://orcid.org/0009-0008-5597-0617
Cómo citar:
Komar, T., Martyniuk, O., Oseredchuk, O., Tsviakh, O., & Borovskyi, V. (2026). Integration of digital technologies in the development of health literacy among higher education students. Revista Eduweb, 20(1), 317-335. https://doi.org/10.46502/issn.1856-7576/2026.20.01.19
Recibido: 16/01/26 Aceptado: 07/03/26
Abstract
Health literacy has become an essential component of personal well-being and professional competence, particularly in the context of the digital transformation of higher education. This study aims to investigate the effectiveness of integrating digital technologies into the development of health literacy among higher education students during their professional training. The research employed a quasi-experimental design combining theoretical, empirical, and statistical methods. The empirical study involved 161 higher education students divided into a control group (80 participants) and an experimental group 0(81 participants). Data were collected through questionnaires and surveys designed to assess three components of health literacy: value-motivational, cognitive, and activity. During the formative stage of the experiment, the experimental group was exposed to a set of pedagogical conditions supported by digital technologies, including online learning platforms, learning management systems, webinars, digital communication tools, and mobile health applications. Statistical analysis was conducted using the Pearson chi-square test to determine the significance of differences between groups. The results demonstrated statistically significant improvements in the level of health literacy among students in the experimental group compared with the control group. The findings indicate that the systematic integration of digital technologies into the educational process contributes to the development of health literacy competencies and supports the formation of health-preserving behaviors among future specialists in higher education.
Keywords: health literacy, digital technologies, future specialists, security sphere, digital space, holistic development of the personality.
Resumen
La alfabetización en salud se ha convertido en un componente esencial del bienestar personal y de la formación profesional, especialmente en el contexto de la transformación digital de la educación superior. El presente estudio tiene como objetivo analizar la efectividad de la integración de tecnologías digitales en el desarrollo de la alfabetización en salud entre estudiantes de educación superior durante su formación profesional. La investigación se desarrolló mediante un diseño cuasi experimental que combinó métodos teóricos, empíricos y estadísticos. El estudio empírico incluyó a 161 estudiantes de educación superior distribuidos en un grupo control (80 participantes) y un grupo experimental (81 participantes). La recolección de datos se realizó mediante cuestionarios y encuestas orientados a evaluar tres componentes de la alfabetización en salud: valor-motivacional, cognitivo y de actividad. Durante la etapa formativa del experimento, el grupo experimental participó en un conjunto de condiciones pedagógicas apoyadas en tecnologías digitales, incluyendo plataformas de aprendizaje en línea, sistemas de gestión del aprendizaje, seminarios web, herramientas de comunicación digital y aplicaciones móviles relacionadas con la salud. El análisis estadístico se realizó mediante la prueba de chi-cuadrado de Pearson para determinar la significancia de las diferencias entre los grupos. Los resultados evidenciaron mejoras estadísticamente significativas en los niveles de alfabetización en salud en el grupo experimental en comparación con el grupo control.
Palabras clave: alfabetización en salud, tecnologías digitales, futuros especialistas, ámbito de la seguridad, espacio digital, desarrollo holístico de la personalidad.
Introduction
In recent decades, health literacy has become an important component of human development and a key factor influencing individual well-being and the quality of professional activity. In the context of rapid technological progress and the digital transformation of society, the formation of health literacy among higher education students is gaining particular relevance. Health literacy is understood as the ability of individuals to obtain, understand, critically evaluate, and apply health-related information in order to make informed decisions that support a healthy lifestyle and maintain physical, psychological, and social well-being (Vuorikari et al., 2022).
The growing digitalization of education significantly expands opportunities for developing health literacy. Digital tools such as online learning platforms, virtual educational environments, mobile applications, and communication technologies enable access to health information, promote interactive learning, and support the development of practical health-related skills (Tai et al., 2022).
Despite the growing body of research, several important gaps remain in the literature. First, many studies focus primarily on general digital health literacy or on specific population groups such as older adults, while relatively little attention is paid to the development of health literacy among higher education students during their professional training. Second, existing research often examines digital technologies as information sources but provides limited empirical evidence regarding their pedagogical effectiveness in structured educational interventions. Third, insufficient attention has been devoted to identifying specific pedagogical conditions that ensure the effective integration of digital technologies into the process of forming health literacy competencies in future specialists (Yin et al., 2019).
These gaps indicate the need for empirical studies that examine how digital technologies can be systematically integrated into higher education to enhance health literacy and health-preserving competencies among students. In particular, it is important to evaluate whether the use of digital educational tools within a structured pedagogical framework contributes to measurable improvements in students’ health literacy levels.
Literature Review
The concept of health literacy has become a central topic in interdisciplinary research at the intersection of education, public health, and digital technologies. The rapid digitalization of society has significantly transformed the ways individuals access, process, and use health-related information. As a result, researchers increasingly emphasize the importance of digital health literacy as a key competency for effective functioning in modern information environments.
One of the main research trends in this field concerns the growing role of digital technologies in improving access to health information and supporting informed health-related decision-making. Studies indicate that digital environments, including online learning platforms, mobile applications, social networks, and virtual educational spaces, can significantly enhance individuals’ ability to obtain and interpret health-related information (Arias López et al., 2023). In addition, digital technologies provide opportunities for interactive learning, personalized information access, and continuous communication between participants in the educational process, which contributes to the development of health-related competencies.
Another important research trend focuses on the relationship between digital inclusion and health literacy. Empirical studies demonstrate that access to digital technologies and the level of digital competence significantly influence the ability of individuals to navigate health information in digital environments. For example, Polonski et al. (2022) investigated the relationship between digital inclusion and health literacy and found that limited access to digital technologies and insufficient digital skills were associated with lower levels of health literacy. These findings highlight the importance of digital competence as a factor influencing the effectiveness of health education initiatives.
Researchers have also explored the pedagogical potential of digital technologies in professional education. Wozniak et al. (2018) analyzed the use of digital tools in health professional education and identified several technologies that significantly influence learning outcomes, including learning management systems, massive open online courses, social media platforms, virtual learning environments, and mobile learning tools. According to the authors, these technologies expand opportunities for collaborative learning, support flexible access to educational resources, and facilitate the development of practical competencies relevant to professional activity.
Technologies for educating a culture of health are based on the formation of ideas about health as a value, on the upbringing of personal qualities in higher education students that constantly contribute to strengthening and preserving their health, increasing responsibility for personal health, strengthening motivation to lead a healthy lifestyle, and family health (Curry & Docherty, 2017).
One of the main innovative forms of student leisure and educational activities is becoming a digital space. Being an active consumer of the digital modern space, a person learns to communicate according to the models provided to them by representatives of mass media. Direct communication disappears from family life in the name of digitalization; the feeling of interaction with others and play are replaced by gadgets (Zhang & Zou, 2020). Children's mastery of digital competence and their safe behavior in the digital space depend largely on parents' and teachers' ability to recognize the risks and opportunities of the digitalization of children's lives. There is an urgent need for parents to develop digital competence as part of their culture, which implies appropriate knowledge of digital technologies and the use of educational platforms, rather than only the appropriate technical level in parents' use of the Internet and computer technology (Galbán & Vidal, 2019).
Modern requirements for training specialists are based on the social demand for health-preserving activities of all specialists; information and communication technologies, new primary digital technologies aimed at the interaction of the teacher and students and the participants of the educational process themselves in order to develop their general human and professional qualities; the need for activities to form human health, strengthen, preserve and update the education of students and form health parity (Fancourt et al., 2016).
Analyzing the problem of health preservation in society, we will form the basic concept of “health preservation competence”. We consider the specified competence an integral quality of the student, manifested in the future specialist's general ability to engage in health preservation activities, grounded in the integration of personal values, abilities, skills, and knowledge to preserve mental, social, physical, and spiritual health. With this approach to the concept, we see the creation of a health-preserving environment in the interests of one’s own health, each student’s health, and society's health, as necessary. To do this, it is necessary to make a transition to health preservation forms of education from traditional ones. The created health preservation educational environment, using modern digital technologies, ensures the development of skills to strengthen and preserve health and fosters positive motivation among students toward a healthy lifestyle. The creation of a healthy environment is of great importance for the holistic development of the individual, as the organization of the educational process enables students to realize their abilities across various fields of activity in such conditions (Mendonça & Sousa, 2025).
Previous studies have applied various methodological approaches to investigate health literacy and digital technologies. Quantitative methods are widely used to assess health literacy levels and examine correlations between digital competence and health outcomes. For instance, large-scale surveys and standardized measurement tools such as the Health Literacy Questionnaire (HLQ) and the eHealth Literacy Scale (eHEALS) have been applied to measure different dimensions of health literacy in diverse populations (Galbán & Vidal, 2019). Cross-sectional studies and statistical analyses have been particularly common in public health research focusing on digital health literacy.
At the same time, qualitative approaches have also been employed to explore individuals’ experiences with digital health information and the ways in which digital environments influence learning and health-related behavior. In educational research, experimental and quasi-experimental designs are increasingly used to evaluate the effectiveness of digital learning tools in developing specific competencies, including health literacy.
Despite the growing number of studies in this area, several methodological and conceptual limitations remain. First, many studies primarily focus on measuring health literacy levels or examining correlations between digital access and health outcomes, rather than evaluating the pedagogical effectiveness of digital technologies in structured educational settings. Second, a significant proportion of research concentrates on specific population groups, such as older adults or healthcare professionals, while relatively little attention has been paid to higher education students as future specialists whose professional activities may influence the health and well-being of others.
Another limitation concerns the insufficient integration of digital technologies into pedagogically grounded models of health literacy development. While many studies acknowledge the potential of digital tools, they often analyze them as isolated technological resources rather than as elements of a comprehensive educational environment supported by specific pedagogical conditions. Consequently, the mechanisms through which digital technologies contribute to the formation of health literacy competencies in higher education remain insufficiently explored.
Furthermore, existing research often presents descriptive analyses of digital tools without providing sufficient empirical evidence regarding their effectiveness in improving students’ health literacy within formal educational contexts. This indicates the need for experimental studies that systematically examine the impact of digital technologies on the development of health literacy during professional training.
Therefore, the present study seeks to address these research gaps by empirically investigating the effectiveness of pedagogical conditions for developing health literacy among higher education students through the integration of digital technologies in the educational process. The study contributes to the existing literature by combining theoretical analysis with experimental research aimed at evaluating the impact of digital learning environments on the formation of health-preserving competencies in future specialists.
Methodology
Research design
The study employed a quasi-experimental research design aimed at evaluating the effectiveness of pedagogical conditions for the development of health literacy among higher education students through the integration of digital technologies in the educational process. The research combined theoretical analysis with empirical investigation and statistical verification of the obtained results.
The experimental study was conducted during 2022–2025 and included two stages: an ascertaining stage, which aimed to determine the initial level of health literacy among students, and a formative stage, during which the proposed pedagogical conditions and digital technologies were implemented in the educational process.
Participants
The empirical study involved 161 higher education students participating in professional training programs. The sample consisted of two independent groups: a control group (CG) comprising 80 participants and an experimental group (EG) including 81 participants. The groups were formed to ensure comparability in terms of educational conditions and initial levels of health literacy.
The sample size was determined using statistical principles that ensure the representativeness of the sample and the reliability of the results. The number of participants in each group exceeded the minimum required level for conducting statistical hypothesis testing.
Instruments and data collection
Data collection was carried out using several empirical methods. Questionnaires and surveys were used to assess the level of students’ health literacy and to identify their attitudes toward health-preserving practices. Document analysis and observation were also applied to evaluate the educational process and students’ engagement with digital learning tools.
The assessment of health literacy was based on three main components:
For each component, three levels of development were identified: low, medium, and high.
Intervention and use of digital technologies
During the formative stage of the experiment, the experimental group was exposed to a set of pedagogical conditions designed to enhance health literacy through digital technologies. These conditions included the integration of digital learning platforms, online educational resources, webinars, virtual learning environments, and digital communication tools into the educational process.
Students in the experimental group participated in interactive online activities, virtual discussions, and educational projects aimed at developing knowledge and practical skills related to healthy lifestyle practices. Digital tools also enabled continuous access to health-related educational materials and supported collaborative learning and communication among participants in the educational process.
Data analysis
The collected data were analyzed using methods of mathematical statistics to verify the reliability and significance of the results. In particular, statistical hypothesis testing was conducted using the Pearson chi-square (χ²) criterion to determine the significance of differences between the control and experimental groups.
Two statistical hypotheses were formulated:
The empirical value of the χ² statistic was compared with the critical value at a significance level of α = 0.05. If the calculated χ² value exceeded the critical value, the null hypothesis was rejected and the alternative hypothesis was accepted, indicating statistically significant differences between the groups.
Ethical considerations
Participation in the study was voluntary, and respondents were informed about the purpose of the research. The data were processed anonymously and used exclusively for scientific purposes.
Results and Discussion
The content and importance of human health for society, and the formation of health literacy through digital technologies, are crucial for future specialists in the holistic development of the personality.
We consider the formation of health literacy of future specialists using digital technologies as a system of influences that are carried out in the process of professional training of students, providing for the updating of the content of academic disciplines, the use of modern innovative digital technologies to strengthen the health-preserving component of the content of education, aimed at forming in students the motivation for a healthy lifestyle, needs and value orientations regarding health preservation, health-preserving activities; acquiring sustainable knowledge on individual topics related to health and the use of digital technologies to obtain knowledge on the problems of a healthy lifestyle and health preservation; reflecting on one's own health-preserving activities, with the aim of further effective professional activity.
Health-preserving technologies can be classified into the following groups: organizational-pedagogical, psychological-pedagogical, educational, preserving, health-improving, health-teaching technologies, and the upbringing of a culture of health.
Organizational and pedagogical technologies eliminate the appearance of hypodynamia and overload and determine the structure of the educational process.
Psychological and pedagogical technologies are associated with the teacher's activities in practical classes and lectures.
Educational technologies are programs that help students develop healthy lifestyle skills, foster a culture of health, and prevent bad habits and diseases (Cardina, 2018).
Advantages of digitalization and the security sector's influence on the formation of health-saving competence in future specialists.
The integration of digital technologies offers several advantages for the formation of health-saving competence among future specialists.
First, digitalization provides quick access to health-related information and educational resources. The use of digital documents, learning materials, and standardized electronic systems facilitates the storage, retrieval, and dissemination of information, which improves the efficiency of educational and professional activities.
Second, digital technologies enhance communication and interaction among participants in the educational process, including teachers, students, and other stakeholders. Digital platforms and electronic resources enable rapid information exchange, collaborative work with documents, and timely access to relevant educational materials.
Third, digitalization contributes to increased productivity and efficiency in the educational process. The use of digital tools, services, and online resources for developing tests, learning tasks, and interactive activities allows educators to optimize time and human resources while improving the quality of learning outcomes (Tai et al., 2022).
Fourth, digital environments provide greater security and reliability in information management, as digital storage systems allow effective protection, backup, and recovery of educational data.
Finally, digital technologies ensure mobility and environmental sustainability. They enable access to educational resources from any location and reduce the need for paper-based materials, thereby supporting sustainable development and environmentally responsible practices (da Silva Sobrinho et al., 2025).
The main elements of the digital space and principles for the formation of health literacy of specialists.
Let us name the main elements of the innovative digital space, which, using digital technologies, is aimed at the formation of health literacy in future specialists:
Let us analyze the most important principles of forming health literacy of future specialists in the process of professional training in higher education:
Experimental study on the formation of health literacy in future specialists using digital technologies.
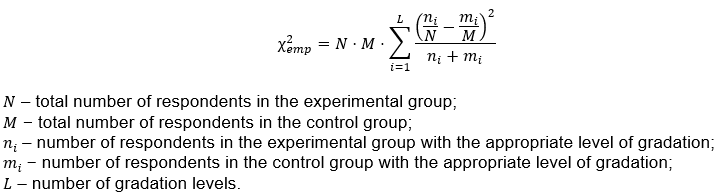
We will describe the methods of statistical processing of empirical data. The study’s general population consists of future specialists. It is advisable to use open data sources to determine its volume. To participate in the experimental study, the required number of respondents was calculated using the formula:

In determining the value (d = 0,5) − d – absolute maximum permissible error.
σ – standard deviation (σ = 2).
Therefore, to ensure the reliability of the experiment, the number of higher education applicants in both the control and experimental groups should be at least 69. As the formula shows, the representativeness of a sample with a smaller general population can be ensured with a correspondingly smaller number of respondents, and the larger the sample size, the more representative it is relative to the general population.
Based on the data of the CG and EG indicators on the results of observations, the empirical value of the criterion was calculated χ²emp, which was compared with that given in the table of critical values χ²α, a reference known number with a given probability of error (significance level 0.05) − the critical value of the criterion χ²crit.
In our study, a 5% probability of error is allowed because the level of probability is set to 0.05; that is, the reliability of the result is 95%.
According to the table, the value of χ²crit is determined for the significance level α=0.05. The degrees of freedom are 4. Therefore, χ²crit = 9,49.
We calculate the empirical value of the χ² criterion using the formula:
Based on the results of comparing the empirical and critical values of the χ² criterion, the following conclusions were made:
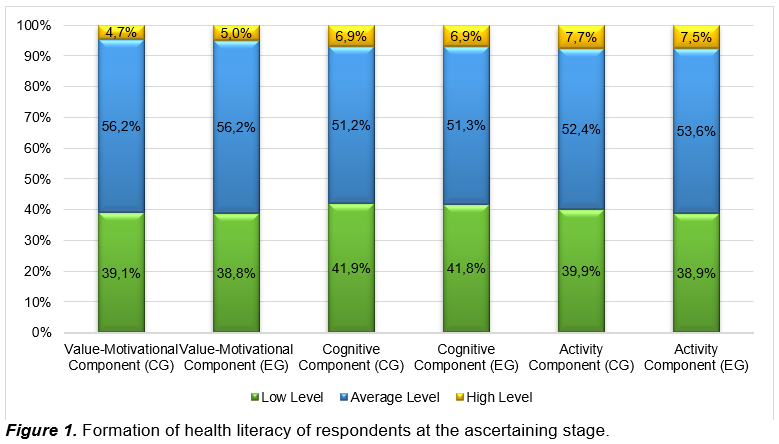
Results of the ascertaining stage of the experiment.
At the ascertaining stage of the experiment, we obtained data that gave grounds for expressing assumptions (preliminary) regarding the formation of students' health literacy:
Respondents in the control and experimental groups revealed approximately the same levels of formation of the outlined components of health literacy.
Let us consider each component of students' health literacy separately.
Diagnosis of the formation of the value-motivational component in respondents showed the following:
Table 1.
Formation of the health literacy of respondents at the ascertaining stage (value-motivational component)

Let us compare the experimental groups – the control group and the experimental group in terms of the level of formation of health literacy in students in relation to the value-motivational component and check the obtained data, in particular, their reliability. To this end, we formulated two hypotheses.
Hypothesis H0: the experimental group and the control group of respondents do not differ significantly in terms of the level of formation of the outlined component of health literacy.
Hypothesis H1: The experimental group and the control group of respondents differ significantly in terms of the level of formation of the outlined component of health literacy.
Let us calculate the Pearson criterion.
χ²emp is less than χ²crit; therefore, the hypothesis H0 is accepted: the experimental and control groups of respondents do not differ significantly in the level of formation of the outlined component of health literacy.
The null hypothesis H0 is accepted: the experimental and control groups of respondents do not differ significantly in the level of formation of the outlined component of health literacy.
Diagnosis of the formation of the following cognitive component of health literacy of respondents revealed the following:
Table 2.
The formation of health literacy of respondents at the ascertaining stage (cognitive component)

Let us compare the level of formation of the cognitive component of health literacy between future specialists in the experimental and control groups and assess the reliability of the obtained data. To this end, we formulated two hypotheses.
Hypothesis H0: The experimental group and the control group of respondents do not differ significantly in the level of formation of the outlined component of health literacy.
Hypothesis H1: The experimental group and the control group of respondents differ significantly in the level of formation of the outlined component of health literacy.
Analogously to the first component, the Pearson criterion was calculated.
The null hypothesis H0 is accepted: the experimental and control groups of respondents do not differ significantly in the level of formation of the outlined component of health literacy.
The diagnosis of the formation of the following activity component of health literacy for future specialists is shown in the table.
Table 3.
Formation of health literacy of respondents at the ascertaining stage (activity component)

Based on the level of formation of the activity component, we will compare the control and experimental groups regarding the health literacy of future specialists and assess the obtained data and their reliability. To this end, two hypotheses were formulated, analogous to the verification of the previous components: Hypothesis H0 and Hypothesis H1. The Pearson criterion was calculated analogously to the previous components.
Hypothesis H0 is accepted: the experimental and control groups of respondents do not differ significantly in the level of formation of the outlined component of health literacy.
Thus, based on the results of the ascertaining stage of the study (Figure 1), it was concluded that there are no statistically significant differences between the control and experimental groups of respondents in the level of formation of individual components of health literacy.
The results of the ascertaining section showed an insufficient level of formation of health literacy of future specialists. We developed and implemented in the EG pedagogical conditions for the formation of the specified competence of future specialists by means of digital technologies:
Results of the formative stage of the experiment.
At the end of the formative stage, we obtained empirical data that allowed us to make the following assumptions about the formation of health literacy in the respondents of the control group and the experimental group:
The formation of the following value-motivational component of health literacy in future specialists is shown in the table.
Table 4.
Formation of health literacy of respondents at the formative stage (value-motivational component)

Let us compare the experimental and control groups in terms of the level of students' health literacy, as measured by the value-motivational component, and assess the reliability of the obtained data.
Let us formulate two hypotheses.
Hypothesis H0: the experimental group and the control group of respondents do not differ significantly in the level of formation of the outlined component of health literacy.
Hypothesis H1: The experimental group and the control group of respondents differ significantly in the level of formation of the outlined component of health literacy.
Let us calculate the Pearson criterion.
The calculated χ²emp exceeds χ²crit; accordingly, the hypothesis H1 is accepted: the experimental and control groups of respondents differ significantly in the level of formation of the outlined component of health literacy.
Let us present the results of the diagnosis of the formation of the cognitive component of respondents' health literacy in the table.
Table 5.
Respondents' health literacy at the formative stage (cognitive component)

Let us compare the experimental and control groups in terms of the level of health literacy formation among future specialists, by cognitive component. Let us check the reliability of the obtained data. Let us formulate two hypotheses, and similarly to the previous component, we will calculate the Pearson criterion.
The calculated χ²emp exceeds χ²crit. Therefore, the hypothesis H1 is accepted: the experimental and control groups of respondents differ significantly in the level of formation of the outlined component of health literacy.
Let us present the diagnosis of the formation of health literacy by the activity component in the table.
Table 6.
The formation of health literacy of respondents at the formative stage (activity component)

Let us compare the experimental and control groups in terms of the level of formation of the activity component of health literacy among respondents and assess the reliability of the obtained data. Let us formulate two hypotheses.
Hypothesis H0: The experimental group and the control group of respondents do not differ significantly in the level of formation of the outlined component of health literacy.
Hypothesis H1: The experimental group and the control group of respondents differ significantly in the level of formation of the outlined component of health literacy.
Similarly to the previous component, we calculate the Pearson criterion.
The calculated χ²emp exceeds χ²crit; therefore, the hypothesis H1 is accepted: the experimental and control groups of respondents differ significantly in the level of formation of the outlined component of health literacy.
The presented data (Figure 2) allow us to conclude that the experimental group, in which the developed pedagogical conditions were implemented, showed significantly better results than the control group regarding the level of formation of all components of health literacy among the respondents.
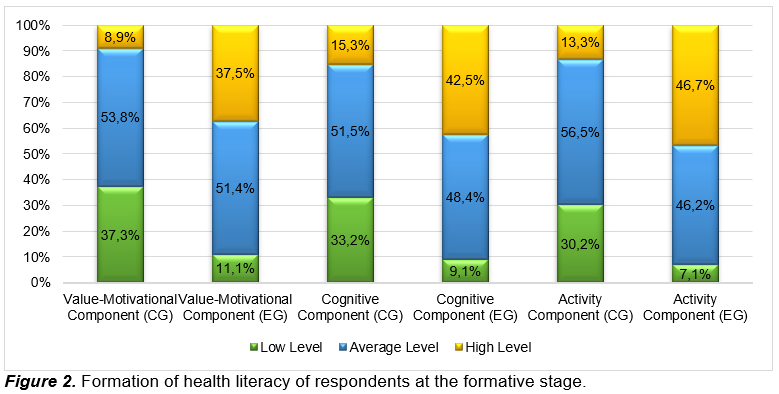
Analysis of the dynamics of the formation of all the identified components of health literacy of future specialists gives grounds to say that in the experimental group, positive changes were expressed to a greater extent than in the control group and that there are statistically significant differences between the experimental and control groups of respondents in terms of the level of formation of both individual components and health literacy in general. We report that more significant positive changes were observed in the experimental group than in the control group, underscoring the importance and effectiveness of the pedagogical conditions for the development of health literacy among future specialists, particularly through digital technologies.
The results of the experimental study demonstrate that the integration of digital technologies into the educational process contributes to improvement in the level of health literacy among higher education students. The analysis of the formative stage of the experiment showed that the proportion of students with high levels of value-motivational, cognitive, and activity components of health literacy increased considerably in the experimental group compared with the control group. These findings indicate the effectiveness of the implemented pedagogical conditions and confirm the positive impact of digital technologies on the development of health-saving competence among future specialists.
The obtained results are consistent with previous studies that emphasize the important role of digital technologies in improving health literacy and access to health-related information. In particular, Arias López et al. (2023) highlight that digital environments significantly expand opportunities for obtaining and processing health information, which contributes to the development of informed health-related decision-making. Similarly, research by Wozniak et al. (2018) shows that digital learning platforms, mobile technologies, and online educational resources enhance students’ engagement and support the development of professional competencies in health-related education. Our findings confirm these conclusions by demonstrating that the systematic integration of digital tools within the educational process can lead to measurable improvements in students’ health literacy levels.
At the same time, the results also complement previous research by providing empirical evidence obtained through an experimental design. While many earlier studies have focused primarily on assessing digital health literacy or examining correlations between digital access and health outcomes, the present study demonstrates how a structured pedagogical intervention based on digital technologies can directly influence the formation of health literacy competencies during professional training.
The observed differences between the experimental and control groups can be explained by several factors related to the educational intervention. First, the use of digital technologies provided students in the experimental group with continuous access to educational materials related to health preservation and healthy lifestyle practices. This increased availability of information may have contributed to the development of the cognitive component of health literacy. Second, interactive learning formats such as online discussions, digital projects, and collaborative tasks enhanced student engagement and motivation, which positively influenced the value-motivational component of health literacy. Third, the use of digital tools and online resources allowed students to apply theoretical knowledge in practical situations, thereby strengthening the activity component of health literacy.
Another possible explanation for the higher results observed in the experimental group is the creation of a more flexible and interactive learning environment. Digital technologies enabled the integration of different forms of learning activities, including individual work, collaborative learning, and self-directed study. Such an environment supports active learning and encourages students to independently search for health-related information, critically evaluate it, and apply it in practice.
Thus, the results of the study demonstrate that the improvement in health literacy observed in the experimental group is closely related to the implementation of the proposed pedagogical conditions and the systematic use of digital technologies in the educational process. Digital tools not only facilitated access to information but also created new opportunities for interaction, collaboration, and practical application of knowledge, which collectively contributed to the development of students’ health-saving competence.
Overall, the findings confirm that the integration of digital technologies into higher education can serve as an effective pedagogical strategy for enhancing health literacy among future specialists and for improving the quality of professional training in modern educational environments.
Limitations
Despite the valuable findings obtained in this study, several limitations should be acknowledged. First, the sample size was relatively limited and consisted of 161 higher education students from specific training programs (psychology, physical education, and border security). Therefore, the results may not be fully generalizable to students from other academic disciplines or educational contexts. Future studies should include a larger and more diverse sample to improve the external validity of the findings.
Second, the study relied primarily on questionnaires and self-reported data to assess students’ levels of health literacy. Although these instruments allowed for the collection of important empirical information, self-assessment may introduce subjectivity and potential response bias. The inclusion of additional objective assessment tools or behavioral indicators of health literacy could strengthen the reliability of the results.
Third, the research focused mainly on the short-term impact of integrating digital technologies within a structured pedagogical intervention. The study did not examine the long-term sustainability of the observed improvements in health literacy. Longitudinal research is therefore needed to determine whether the positive effects of digital learning environments persist over time.
Finally, the study examined the overall effectiveness of digital technologies without differentiating the specific impact of individual digital tools or platforms used in the educational process. Future research could analyze the effectiveness of particular digital technologies or instructional strategies in greater detail in order to identify the most effective approaches for developing health literacy among higher education students.
RECOMMENDATIONS for higher education teachers on implementing targeted work on the formation of health literacy of future specialists:
Future Research Directions
Future research may expand the study of health literacy development among higher education students through digital technologies by involving larger and more diverse samples from different academic disciplines and educational contexts. This would allow for a broader generalization of the obtained results.
Another important direction is the investigation of the long-term effects of integrating digital technologies into the educational process in order to determine the sustainability of improvements in students’ health literacy.
In addition, further studies may focus on analyzing the effectiveness of specific digital tools and educational strategies (such as mobile applications, virtual environments, or gamified learning) for developing health-preserving competencies in future specialists.
Conclusions
The study provides empirical evidence of the effectiveness of integrating digital technologies into the educational process for the development of health literacy among higher education students. The experimental results demonstrated statistically significant improvements in the value-motivational, cognitive, and activity components of health literacy in the experimental group compared with the control group. These findings confirm that the implementation of structured pedagogical conditions supported by digital technologies contributes to the formation of health-preserving competencies among future specialists.
The main empirical contribution of the study lies in the experimental verification of pedagogical conditions that integrate digital tools into professional training in higher education. The research demonstrates that the systematic use of digital educational platforms, interactive online activities, and digital communication tools can significantly enhance students’ motivation toward a healthy lifestyle, expand their knowledge about health preservation, and strengthen their ability to apply this knowledge in practice.
The findings also have important practical implications for higher education institutions. In particular, universities may incorporate digital learning platforms, mobile health applications, virtual learning environments, and interactive digital resources into the curriculum to support the development of students’ health literacy. In addition, the results highlight the importance of modernizing educational programs, increasing practical digital learning activities, and improving teachers’ digital competencies in order to create a supportive educational environment that promotes health-preserving behaviors among students.
Bibliographic references
Arias López, M. del P., Ong, B. A., Borrat Frigola, X., Fernández, A. L., Hicklent, R. S., Obeles, A. J. T., Rocimo, A. M., & Celi, L. A. (2023). Digital literacy as a new determinant of health: A scoping review. PLOS Digital Health, 2(10), e0000279. https://doi.org/10.1371/journal.pdig.0000279
Cardina, C. (2018). Professional development activities and support among secondary health teachers. Pedagogy in Health Promotion, 4(3), 190–199. https://doi.org/10.1177/2373379917742924
Carrasco-Dajer, C. M., Vera-Calzaretta, A. R., Ubillos-Landa, S., Oyanedel, J. C., & Díaz-Gorriti, V. (2024). Impact of a culturally adapted digital literacy intervention on older people and its relationship with health literacy, quality of life, and well-being. Frontiers in Psychology, 15, 1305569. https://doi.org/10.3389/fpsyg.2024.1305569
Collet, G. D. O., Ferreira, F. D. M., Ceron, D. F., Fracasso, M. D. L. C., & Santin, G. C. (2024). Influence of digital health literacy on online health-related behaviors influenced by internet advertising. BMC Public Health, 24(1), 1949. https://doi.org/10.1186/s12889-024-19506-6
Curry, L., & Docherty, M. (2017). Implementing competency-based education. Collected Essays on Learning and Teaching, 10, 61–73. https://files.eric.ed.gov/fulltext/EJ1147189.pdf
da Silva Sobrinho, A., da Silva Rodrigues, G., de Oliveira, G., de Oliveira Gomes, G., & Bueno Júnior, C. (2025). Everyday digital support to promote health and literacy among older adults: 14-week randomized digital pilot trial by engagement level. JMIR Formative Research, 9, e77319. https://doi.org/10.2196/77319
Fancourt, D., Perkins, R., Ascenso, S., Carvalho, L. A., Steptoe, A., & Williamon, A. (2016). Effects of group drumming interventions on anxiety, depression, social resilience and inflammatory immune response among mental health service users. PLOS ONE, 11(3), e0151136. https://doi.org/10.1371/journal.pone.0151136
Galbán, P. A., & Vidal, N. V. (2019). Digital literacy program for the use of social media, aimed at health professionals. In L. Ohno-Machado & B. Seroussi (Eds.), MEDINFO 2019: Health and wellbeing e-networks for all (Vol. 264, pp. 1895–1896). Studies in Health Technology and Informatics. https://doi.org/10.3233/SHTI190701
Mendonça, A. V. M., & Sousa, M. F. de. (2025). Desafios contemporâneos para a saúde digital: Letramento, educação midiática e prevenção à desinformação. Revista Panamericana de Salud Pública, 49, e14. https://doi.org/10.26633/RPSP.2025.14
Polonski, T. C., Zanin, L., Oliveira, A. M. G., Dutra, E. R., Silva Filho, D. A. da, & Flório, F. M. (2022). Influência da inclusão digital na alfabetização em saúde de idosos. ETD – Educação Temática Digital, 24(3), 584–597. https://doi.org/10.20396/etd.v24i3.8661696
Tai, T.-Y., Chen, H. H.-J., & Todd, G. (2022). The impact of a virtual reality app on adolescent EFL learners’ vocabulary learning. Computer Assisted Language Learning, 35(4), 892–917. https://doi.org/10.1080/09588221.2020.1752735
Vuorikari, R., Kluzer, S., & Punie, Y. (2022). DigComp 2.2: The digital competence framework for citizens: With new examples of knowledge, skills and attitudes (EUR 31006 EN). Publications Office of the European Union. https://doi.org/10.2760/115376
Wozniak, H., Ellaway, R. H., & de Jong, P. G. M. (2018). What have we learnt about using digital technologies in health professional education? The Medical Journal of Australia, 209(10), 431–433.e1. https://doi.org/10.5694/mja18.00152
Yin, H., Huang, S., & Chen, G. (2019). The relationships between teachers’ emotional labor and their burnout and satisfaction: A meta-analytic review. Educational Research Review, 28, 100283. https://doi.org/10.1016/j.edurev.2019.100283
Zhang, R., & Zou, D. (2020). Types, purposes, and effectiveness of state-of-the-art technologies for second and foreign language learning. Computer Assisted Language Learning, 35(4), 696–742. https://doi.org/10.1080/09588221.2020.1744666

Este artículo no presenta ningún conflicto de intereses. Este artículo está bajo la licencia Creative Commons Atribución 4.0 Internacional (CC BY 4.0). Se permite la reproducción, distribución y comunicación pública de la obra, así como la creación de obras derivadas, siempre que se cite la fuente original.